Marfan syndrome (MFS) is a genetic disorder of the body’s connective tissue that affects any gender, race or ethnic group.
Connective tissue helps provide structure to the body, binding skin to muscle and muscle to bone. It provides the stretchy strength of tendons and ligaments around joints, and in blood vessel walls. It also supports the internal organs. This tissue is made of fine fibres and ‘glue’. One fibre is called fibrillin. In MFS, a change in the fibrillin-producing gene, fibrillin-1, means that this protein is deficient in connective tissue throughout the body, creating an unusual stretchiness and weakness of tissues.
This has far-reaching implications and can affect the eyes, lungs, gut, nervous system, skeleton and, most dangerously, the cardiovascular system.
Symptoms can vary widely from person to person with people experiencing mild to severe manifestations.
MFS affects roughly 1 in 3,000 people which means that approximately 18,000 people in the UK have MFS. We estimate that half remain undiagnosed.
75% of people inherit the condition whilst 25% develop it as a result of a spontaneous (new) gene change. Each child of an affected parent has a 50% chance of inheriting Marfan syndrome.
View resources on Marfan Syndrome
Marfan syndrome can be difficult to diagnose because signs of the condition vary greatly from person to person. MFS is multi-faceted and most affected people will not have all the signs and complications of the syndrome. The most common, visible feature is excessive height with disproportionally long limbs, fingers and toes. This is sometimes accompanied by a protruding or indented chest, curved spine (scoliosis), high-arched palate, crowded teeth, shortsightedness and dislocated eye lenses.
An early, accurate diagnosis is essential, not only for people with Marfan syndrome but also related connective tissue disorders. MFS belongs to a wider family of connective tissue disorders that includes Loeys-Dietz syndrome. Early accurate diagnosis of MFS can be confirmed by genetic testing. The Trust helped to set up Marfan clinics in 24 NHS regional genetic centres in the United Kingdom, click here for the link to the list. Referral to your nearest centre can be obtained through your GP. Genetic testing involves the analysis of a blood sample for a change in the fibrillin-1 gene.
Preimplantation Genetic Diagnosis (PGD) is available, if one parent is affected. This is a technique that can test embryos for the gene change before they are implanted in the womb to ensure the baby is unaffected.
A clinical diagnosis is also possible after careful physical examination by an experienced doctor if there are numerous signs, specifically those of aortic dilatation and dislocated eye lenses, especially if a person has a known family history of Marfan syndrome. However, genetic testing is increasingly used to test patients and has become the most definitive diagnostic tool which can be used in conjunction with other tests and assessments.
Know the Signs of Marfan Syndrome
Skeleton:

Musculoskeletal problems are common and troublesome in MFS, with patients often growing to excessive height while developing curvature (scoliosis/kyphosis/ lordosis) of the spine. Fingers are often spidery and long, and hammer toes are a frequent feature. Skeletal problems also involve abnormally shaped chest (pectus deformity), and loose joints which frequently cause pain and occasionally joint dislocation.
Heart:
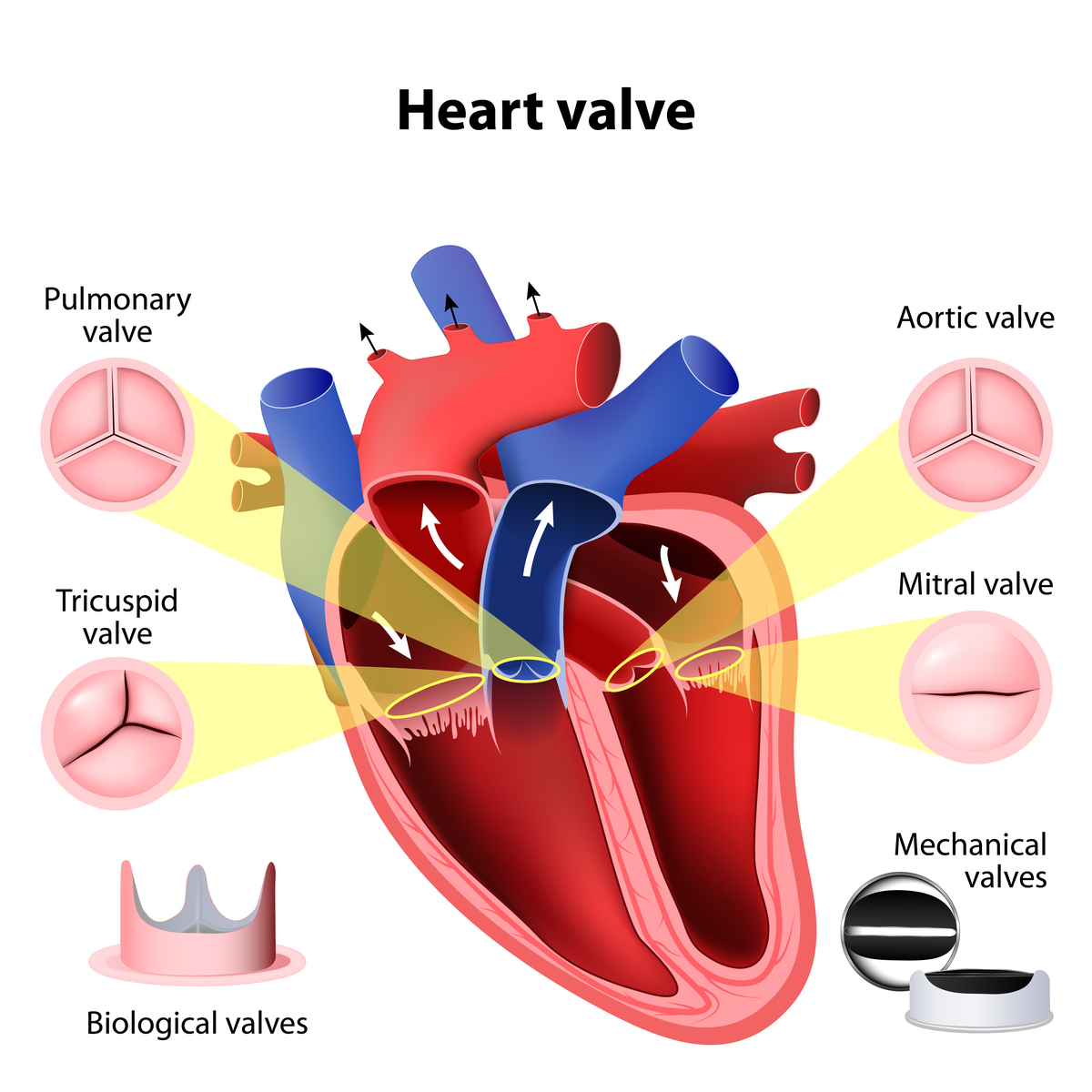
People can experience ballooning and potentially fatal tearing of the aorta (the body’s largest artery, carrying oxygen-rich blood from the heart to the circulatory system) and backward billowing of the heart’s valves. Left unmonitored or untreated, these symptoms can be life-threatening. The key to a long and healthy life with Marfan syndrome is monitoring with regular scans to check the heart function and the size of the aorta. A combination of echocardiograms and MRI or CT scans are usually used. This allows doctors to plan any treatment that may be required.
Eyes:
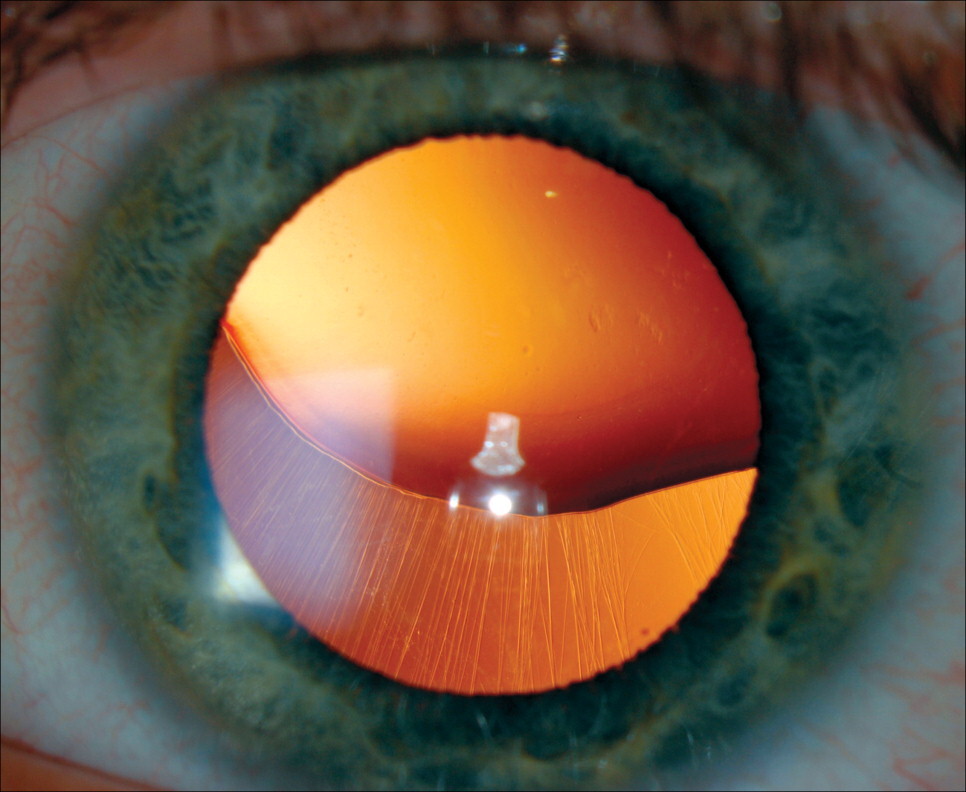
People with MFS are often myopic (short-sighted), with some experiencing dislocation of the ocular lens, and retinal detachment. Strabismus (squint) and glaucoma are also ocular signs.
Dental:
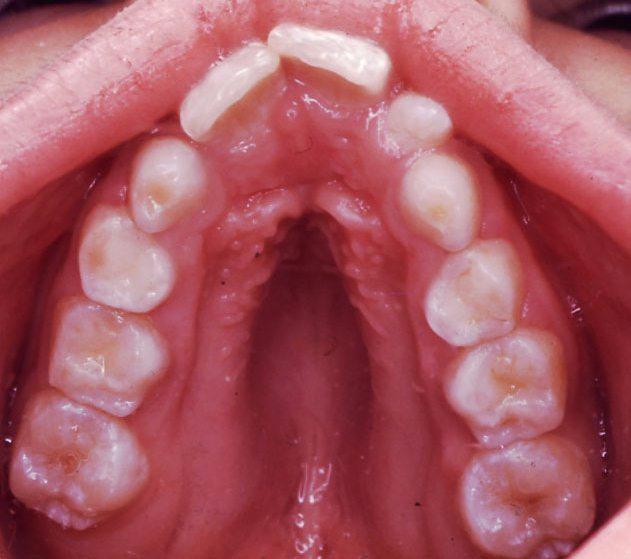
A high-arched palate and crowding of teeth with a history of tooth extraction for crowding is fairly common amongst Marfan patients.
Lungs:
Pulmonary complications occur in 10% of patients, commonly cystic changes in the lung, and occasionally pneumothorax (air trapped outside the lung due to an air leak).
Knowing the signs of Marfan syndrome can therefore save lives. Experts in Marfan syndrome estimate that nearly half the people who have the condition don’t know it. This is something we are working hard to change by raising greater awareness. See our page which details the signs of Marfan syndrome.
For More Information, see:
- The Marfan syndrome section on our Resources page which has detailed information on being diagnosed and living with Marfan syndrome
- What is Marfan Syndrome by Dr Anne Child MD FRCP
- video below "Standing Tall - What is Marfan syndrome and the Marfan Trust" by Tyler Tapping and Cameron McGarry



